Influência da comorbidade entre depressão e transtornos por uso de álcool nos comportamentos suicidas no Estudo de Área de Captação de São Paulo, Brasil*
Revista Brasileira de Psiquiatria
Influência da comorbidade entre depressão e transtornos por uso de álcool nos comportamentos suicidas no Estudo de Área de Captação de São Paulo, Brasil*
Bruno Mendonça CoêlhoI,II; Laura Helena AndradeI; Francisco Bevilacqua GuarnieroI; Yuan-Pang WangI
ISection of Psychiatric Epidemiology (LIM-23), Institute and Department of Psychiatry, School of Medicine, Universidade de São Paulo (USP), São Paulo, SP, Brazil
IIDepartment of Psychiatry, Faculdade de Medicina do ABC, Santo André, SP, Brazil
ABSTRACT
OBJECTIVE: To investigate in a community sample the association of suicide-related cognitions and behaviors (“thoughts of death”, “desire for death”, “suicidal thoughts”, and “suicidal attempts”) with the comorbidity of depressive disorders (major depressive episode or dysthymia) and alcohol or substance use disorders.
METHOD: The sample was 1464 subjects interviewed in their homes using the Composite International Diagnostic Interview to generate DSM-III-R diagnosis. Descriptive statistics depicted the prevalence of suicide-related cognitions and behaviors by socio-demographic variables and diagnoses considered (major depressive episode, dysthymia, alcohol or substance use disorders). We performed a multivariate logistic regression analysis to estimate the effect of comorbid major depressive episode/dysthymia and alcohol or substance use disorders on each of the suicide-related cognitions and behaviors.
RESULTS: The presence of major depressive episode and dysthymia was significantly associated with suicide-related cognitions and behaviors. In the regression models, suicide-related cognitions and behaviors were predicted by major depressive episode (OR = range 2.3-9.2) and dysthymia (OR = range 5.1-32.6), even in the presence of alcohol use disorders (OR = range 2.3-4.0) or alcohol or substance use disorders (OR = range 2.7-2.8). The interaction effect was observed between major depressive episode and alcohol use disorders, as well as between dysthymia and gender. Substance use disorders were excluded from most of the models.
CONCLUSION: Presence of major depressive episode and dysthymia influences suicide-related cognitions and behaviors, independently of the presence of alcohol or substance use disorders. However, alcohol use disorders and gender interact with depressive disorders, displaying a differential effect on suicide-related cognitions and behaviors.
Descriptors: Suicide; Depression; Dysthymic disorder; Alcohol-related disorders; Comorbidity.
RESUMO
OBJETIVO: Investigar, numa amostra comunitária, a associação entre cognições e comportamentos relacionados ao suicídio (“pensamentos de morte”, “desejo de morte”, “pensamentos suicidas”, e “tentativas de suicídio”) e a comorbidade entre transtornos depressivos (episódio depressivo maior ou distimia) e transtornos por uso de álcool ou substâncias.
MÉTODO: 1.464 sujeitos foram entrevistados em seus domicílios com o CIDI para gerar diagnósticos DSM-III-R. Estatística descritiva demonstrou a prevalência de cognições e comportamentos relacionados ao suicídio pelas variáveis sociodemográficas e diagnósticos considerados (episódio depressivo maior, distimia, transtornos por uso de álcool ou substâncias). Realizamos também análises de regressão logística multivariada para estimar o efeito da comorbidade entre episódio depressivo maior/distimia e transtornos por uso de álcool ou substâncias em cognições e comportamentos relacionados ao suicídio.
RESULTADOS: A presença de episódio depressivo maior e distimia foi significativamente associada a cognições e comportamentos relacionados ao suicídio. Em modelos de regressão multivariada, os preditores de cognições e comportamentos relacionados ao suicídio foram episódio depressivo maior (OR range = 2,3-9,2) e distimia (OR range = 5,1-32,6) mesmo na presença de transtornos por uso de álcool (OR range = 2,3-4,0) ou transtornos por uso de substâncias (OR range = 2,7-2,8). O efeito de interação foi observado entre episódio depressivo maior e transtornos por uso de álcool, bem como entre gênero e distimia. Transtornos por uso de álcool foi excluído da maioria dos modelos.
CONCLUSÃO: A presença de episódio depressivo maior e distimia influencia os CCS, independentemente da presença de transtornos por uso de álcool ou substâncias. Contudo, transtornos por uso de álcool e gênero interagem com os transtornos depressivos, demonstrando um efeito diferencial em cognições e comportamentos relacionados ao suicídio.
Descritores: Suicídio; Depressão; Transtorno distímico; Transtornos relacionados ao uso de álcool; Comorbidade.
Introduction
The association of suicide-related cognitions and behaviors (SCB), and psychiatric disorders is well established in psychiatric literature, and there is a corpus of serious publications demonstrating that, among cases of suicide, approximately 90% of individuals had one or more psychiatric disorders at the time they committed suicide.1 Nonfatal SCB (suicidal thoughts, ideation, plans and attempts) are important for public health because they are viewed as powerful predictors of subsequent death by suicide.2-4 Generally, SCB occurs on a continuum of severity and frequency, ranging from the most prevalent and less serious through less prevalent and gradually more severe behaviors. In some individuals, those behaviors may progress all the way through to enduring, intense death ideation, suicide plans and self-inflicted injury without any serious intent to die, and, in a few people, to attempt or complete suicide.5 Therefore, nonfatal suicidal behaviors cause considerable distress and are substantial outcomes in their own right.4
Although data on suicidality consider individual disorders, in general,4,6-8 psychiatric disorders tend to be comorbid and cases that meet criteria for a single psychopathology are rare.9,10 The scientific interest in comorbid psychiatric diagnoses and suicidality is largely based on observations of clinical samples, where patients seeking help with both an internalizing mental disorder and an externalizing alcohol or substance use disorder (AUD/SUD) present a more persistent course, frequent relapses, severe psychopathology, and non-adherence to treatment compared to those with single disorders.11,12 In clinical settings, studies have shown that depression and AUD tend to co-occur in the same patient and will increase the risk of “suicide attempt”, when compared with depressed patients without co-occurring AUD.6,13 In addition, cross-sectional studies in population-based samples found that mental disorders and SUD co-occur at levels much higher than suggested by chance.9,14-17 While clinical evidence of the association of suicidality with comorbid depression and AUD/SUD should not be extended to the general population, less information is available for non-clinical samples.
Almost all major disorders have been associated with SCB and the comorbid nature of several disorders may intensify the association with SCB.4,9 However, few studies have explored the complex nature of comorbid depression and AUD/SUD on suicidality, as well as the interaction effect of the phenomenon of comorbidity.4,6Among groups of psychiatric disorders, mood disorders (depressive and bipolar disorders), alcohol/substance use disorders (AUD/SUD), and psychosis are some of the most frequent diagnoses observed in suicidal individuals.2,7,8,18 Several psychological and neurobiological hypotheses have been raised to account for the link between these psychiatric disorders and the outcome of death by suicide.6,19,20 Therefore, the understanding and clinical treatment of these disorders are of paramount importance for public health interventions that aim to reduce this unfavorable, yet preventable, outcome.
Generally, the relationship between psychiatric morbidities and suicide risk has been established by a bivariate association between psychiatric risk variable and dependent variable, i.e., depressive disorders, AUD, and SUD seem to be independently associated with increased risk of suicide.4,21 The crude odds resulting from the bivariate approach could give only a limited view of the effect of psychiatric comorbidity on SCB, as most relationships between co-variates and suicidality cannot be directly measured. In population-based samples, the relationship between comorbid disorders and SCB is poorly understood. As a consequence, there is a gap in the literature on suicidology that accounts for the concurrent influence of comorbid psychiatric disorders from a multivariate perspective, a view that can provide a more comprehensive explanation of suicide-related phenomena.9,21 Although genetic factors might be implicated in most of the observed comorbidity profile among disorders in pairs of individuals,22 these disorders seem to be the consequence of a predictable contribution of common liability factors. Multivariate methods can be used to demonstrate a better model between internalizing and externalizing liability factors in relation to disorders such as major depressive disorder/dysthymia and AUD/SUD.4,10,13 In addition, most studies regarding the association between mental disorders and SCB were conducted with clinical samples and in developed countries, preventing generalization of the findings. Accordingly, the importance of performing such a study in a Latin American country like Brazil is reinforced by recent data suggesting that mental disorders are less predictive of SCB in developing countries.4
The present article aims to explore the relationship between comorbid depressive disorders, non-affective psychosis and AUD/SUD with nonfatal suicidal cognitions and behaviors. We analyzed: (1) the demographic correlates of SCB and, (2) the association between SCB with depressive disorders (major depressive episode [MDE] or dysthymia) and non-affective psychosis with AUD/SUD in a community sample, with data from an epidemiologic catchment area study in the city of São Paulo, Brazil. Our hypotheses are: (1) MDE and dysthymia, as well as non-affective psychosis, are major predictors of SCB and, (2) the comorbidity of these disorders with AUD/SUD may interfere in these associations.
Method
1. Sampling
Data are from the Sao Paulo Epidemiological Catchment Area Study, a cross-sectional survey which evaluated a representative sample of non-institutionalized individuals aged 18 years or older, living in two boroughs of the Catchment Area of the Medical Center of the Universidade de São Paulo, in the city of São Paulo, Southeast Brazil.23 At the time of the survey (1994-1995), the population living in this area was estimated to be 91,276.24
The sample consists of a household survey using an area probability design with stratification based on age and multiple respondents per household. The sample size for this study was calculated using a 0.05 level two-sided test aiming at a precision of two standard errors (SE) for a rare outcome. To convey the complex sampling design, a list of all individuals living in each selected household was then created. In order to improve the probability of observing both young psychotics and psychiatric morbidity associated with old age, all persons aged 18-24 years and 60 years or older living in each selected household were interviewed. Of the remaining individuals aged 25-59 years living in the selected household, one was chosen for interview based on the Kish selection table.25 In this way, it was possible to have more than one person interviewed in each selected household. The final sample comprised 1,464 subjects, with a response rate of 76.8%. Face-to-face interviews were conducted after the respondents had signed a written informed consent form (Ethical committee approval number 125/93,).
2. Assessment procedure
The instrument used to assess psychiatric diagnosis was the Brazilian version of the Composite International Diagnostic Interview (CIDI),26,27 version 1.1, applied by trained interviewers. This instrument produces psychiatric diagnoses according to DSM-III-R criteria. For the present analysis, four diagnostic categories were considered: lifetime MDE (unipolar or bipolar depression), dysthymia, AUD, and SUD, with the prevalence for each of the categories being, respectively, 16.8%, 4.3%, 5.5%, and 1.1%.23 The lifetime prevalence rate for the total sample for any disorder was 33.1%. We considered AUD and SUD as summary categories for alcohol and substance dependence and abuse.
Lifetime SCB, i.e., “thoughts of death”, “desire for death”, “suicidal thoughts” (cognitions), and “suicide attempts” (behavior) were assessed respectively by four questions of the Suicidality Module of CIDI:26,27 (1) “Has there ever been a period of two weeks or more when you thought a lot about death – either your own, someone else’s, or death in general?”; (2) “Has there ever been a period of two weeks or more when you felt like you wanted to die?”; (3) “Have you ever felt so low that you thought about committing suicide?”; and (4) “Have you ever attempted suicide?”.
3. Statistical analysis
In view of the fact that the data we use were obtained from a complex stratified sample design, they were weighted to adjust for differential probabilities of selection and non-response. The calculation of weight also considered the following factors: (1) the probability of household selection was systematic and is constant for each household unit, as the selection of household was systematic; (2) the probability of selection of each individual in the household. The probability of selection of a subject to be interviewed varies according to age stratum. For stratum 2, the probability is 1/n2i, where n2i represented the number of people aged 25-59 years living in a household. For strata 1 and 3, because everyone aged 18-24 years and aged 60 years or more living in the household was selected for the study, the probability is 1. To find out more about the population’s characteristic gender and regional geographic groupings in the sample age range, post-stratification was also carried out in order to compensate for discrepancies between the original census population data and our sample. For this process, we constructed, taking into account eight age groups and gender, 16 classes for each geographic region. In order to calculate the final weight, a matrix was constructed with the following factors: gender, age, number of persons in each stratum by household, age strata, and a post-stratification factor. Additional information about methodology and sampling has been reported elsewhere.23
The lifetime prevalence of each SCB outcome was calculated for the total sample, by socio-demographic variables (gender, marital status, age group, and educational level), and psychiatric diagnosis (MDE, dysthymia, non-affective psychosis, AUD and SUD). Marital status was coded as currently married, previously married, and never married; age strata were divided into subgroups of 18-34, 35-54 and > 55 year old; and educational level as less than high school, high school, and some form of higher education.
With the purpose of investigating the effect of socio-demographic variables and a specific profile of psychiatric comorbid disorders (MDE, dysthymia or non-affective psychosis with AUD or SUD) in predicting each of the four levels of SCB, logistic regression analyses were performed. First, we calculated crude odds ratio (OR) of independent variables for each SCB.
In order to address the non-independence of data for multivariate models, we tested first the interaction effect, without dropping the main effects. The SAS’ PROC GENMOD statement with the “repeated” statement was used to deal with the possible correlation among individuals within the same family. The method is based on a generalized estimation equations (GEE)28,29 approach for correlated binary responses to model the differences in frequency for each suicidal outcome. The exchangeable correlation option of the GEE was used in the estimation of the parameters for these models, assuming the correlation between any member of the same family to be equal, but “robust standard errors” for regression parameters estimators were requested.
As the second step (Model 1 for each outcome), complex models were used in predicting each SCB, which were performed by backward method, keeping in the model only those variables and interactions that significantly (p < 0.05) contributed to the equation. Demographic variables were considered in all models: gender, marital status, age group and educational level. The model starts by considering MDE as the main predictor, controlling for all demographic variables and the interaction with gender, due to the differential effect of gender in SCB.
In the next step, AUD was considered as the effect of modification in the presence of MDE (Model 2). In this step, we tested two-way interaction: 1) between MDE and AUD; 2) between gender with other socio-demographic variables, 3) between gender and each one of the two disorders considered (MDE and AUD), and 4) three-way interaction between gender, MDE and AUD, also entered in this model. Finally, a new model (Model 3) was adjusted by changing AUD to SUD in the presence of MDE. The same procedures as those described above were repeated considering dysthymia and also non-affective psychosis, instead of MDE, as the main predictor of SCB outcomes. A total of 12 models were built and analyzed for each psychiatric diagnosis.
The goodness-of-fit of the final model, in respect to the largest model in each outcome, was calculated by Wald’s χ2 testing the removal of all deleted terms through the backward procedure. The largest models considered were the one with the demographic and psychiatric variables, with the interaction between gender and all other variables, as well as the three-way interaction of gender*depression/dysthymia/non-affective psychosis*AUD/SUD. Since the models 1, 2 and 3 for each SCB were not built under the assumption of being nested we reported the overall goodness-of-fit χ2 statistics of the final model against the full model of every tested diagnosis. The value of χ2 should be non-significant to demonstrate the simultaneous non-contribution of the terms.
All evaluations were based on two-sided tests (0.05 level of significance). Confidence intervals (CI 95%) of the estimates of regression coefficients were computed using the Jackknife Repeated Replications method (JRR) to adjust for the design effects introduced by the clustering and weighting of observations. Multivariate significance was evaluated with Wald’s χ2 test based on design-corrected coefficient variance-covariance matrices. Analysis was performed through SAS 9.1 software.30
Results
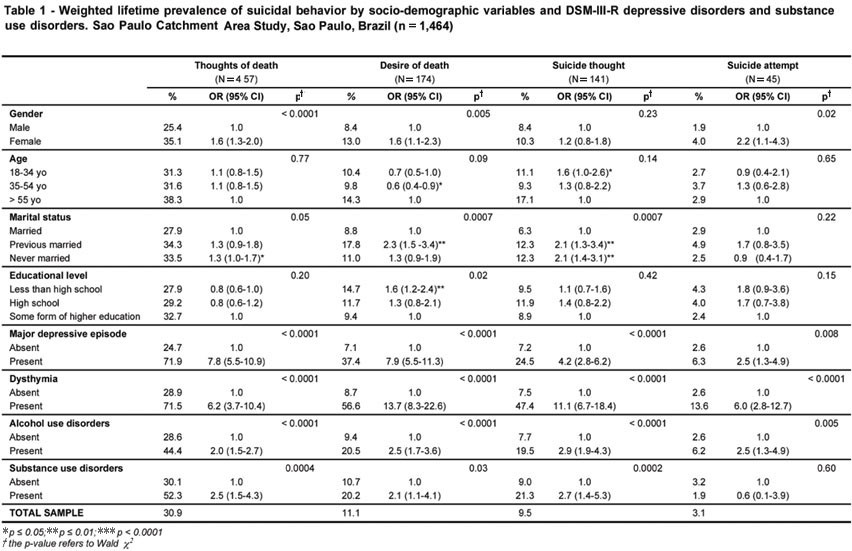
Table 1 shows the lifetime prevalence and crude association of SCB by socio-demographic variables and DSM-III-R categories: MDE, dysthymia, AUD and SUD. Approximately one out of three subjects reported lifetime “thoughts of death”. “Desire for death” and “suicidal thoughts” were found to be present in around 10% of the sample and only one out of 10 individuals with SCB reported a “suicide attempt” (3.1%).
{kind=link}
Three SCB were more frequent in women, with the exception of “suicidal thoughts”, without gender difference in this cognition. Women were twice as likely than men to attempt suicide. Age was not associated with suicidality in this sample. Previously or never married subjects displayed significantly more suicidal cognition, such as “desire for death”. They were twice as likely to report “suicidal thoughts” when compared to those who were married. Individuals with less than a high school education presented more “desire for death” (OR = 1.6; 95% CI 1.2-2.4). In this descriptive analysis, MDE and dysthymia emerged as determinants of all SCB, with unadjusted OR ranging from 2.5 to 13.7. AUD and SUD were associated with SCB, with the exception that SUD was not associated with “suicide attempts”. Non-affective psychosis was associated with all SCB except “suicide attempt” (data not shown).
Twelve multivariate logistic regression models were built to estimate the effect of psychiatric diagnosis (MDE and dysthymia) controlled for demographic variables for each SCB. All three-way interactions of depressive disorders, gender and AUD/SUD were removed after adjustment. Due to the lack of significant effect of most SUD-related models, they are not displayed in the tables (Tables 2 to 5). Additionally, Wald’s χ2 for model fit was also shown and, with just one exception in model 1 for dysthymia and “suicidal thoughts” (Table 5), the final models were not significantly different from the largest model for each outcome.
1. Major depressive episode as predictor for SCB
Table 2 shows the models for “thoughts of death” and “desire for death”. The cognition of “thoughts of death” was predicted in all models by female gender (OR range = 1.4-1.7). In model 2, one could observe an interaction between MDE and AUD (OR range = 0.8 to 8.9). In this same model, AUD also emerged as significant: OR = 2.7 (95% IC 1.7-4.0).The adjusted model 3 also showed that SUD was associated with “thoughts of death” (OR = 2.8; (95% CI 1.4-5.6).
For the “desire for death”, low educational attainment (OR range = 2.4-2.6), and MDE (OR range = 9.0-9.2) were significantly associated in model 1 and 2. In addition, AUD was significantly associated with this cognition (OR = 2.5; 95% CI 1.5-4.1). Gender and SUD (not displayed) were not associated with this SCB. No two- or three-way interactions for “thoughts of death” and “desire for death” were found.
The likelihood of having “suicidal thoughts” also was outstanding for marital status (OR = 1.9-2.2) and MDE (OR range = 4.0-4.3), whereas AUD also displayed considerable effect (OR = 2.5; 95% CI 1.5-4.1). However, female gender and SUD were excluded from all models for this suicidal cognition (Table 3).
In the model for “suicide attempts” (Table 3), the association of MDE with this nonfatal suicidal behavior ranged from OR = 2.3-2.4. Other predictors for model 2 were: low and intermediate educational attainment (OR = 3.2 and 3.8, respectively), and AUD (OR = 4.0; 95% CI 1.7-9.6). Depressive males presented interaction with the adult age group (35-54 years old.) with OR ranging from 8.9 to 14.6, whereas females were not associated with this SCB. SUD have shown no effect in the tested model. There were no two- or three-way interactions for “suicidal thoughts” or “suicide attempts”.
2. Dysthymia as predictor for SCB
The effect of dysthymia on all SCB models was similar to MDE and the effect of SUD was observed only for “thoughts of death”. In this SCB, in comparison with MDE, some slight difference was observed for adjusted models of dysthymia and no interaction effect emerged. Table 4 shows that “thoughts of death” was predicted by female gender (OR range = 1.6-1.8), dysthymia (OR range = 5.6-6.0), AUD (OR = 2.3; 95% CI 1.6-3.4), and SUD (OR = 2.7; 95% CI 1.4-5.1).
The likelihood of having “desire for death” was significant for the female gender only in model 2 (OR = 2.0; 95% IC 1.3-3.1), and dysthymia (OR range = 12.6 and 14.0). In addition, previously married individuals (OR = 1.8 in the model 1) and AUD (OR = 2.9; 95% CI 1.8-4.7, in model 2) also emerged as significantly associated with this cognition (Table 4). SUD respondents showed no effect in the model for “desire for death”. Once again, neither the models for “thoughts of death” nor “desire for death” for dysthymia presented any two- or three-way interactions.
Table 5 shows models 1 and 2 for “suicidal thoughts” and “suicide attempts”, as SUD had no effect on these two SCB. Concerning “suicidal thoughts”, marital status (OR range = 1.6-2.4) and AUD (OR = 2.7; 95% CI 1.7-4.5, for model 2) emerged as a predictor. An interaction effect was also observed between dysthymia and gender. In model 1, dysthymic males presented OR = 32.6 while females presented OR = 6.9. When AUD was entered into model 2, OR for dysthymic males was 31.0 and for females was 6.2.
For “suicide attempts” (Table 5), dysthymia (OR = 5.1 and 5.9) significantly predicted this SCB. While AUD showed a consistent effect on this behavior (OR = 3.9; 95% CI 1.7-9.0), SUD was eliminated in model 3. In model 2, low and intermediate educational level were also predictors for this SCB (OR = 3.4 and 3.0, respectively). As for MDE, gender presented an interaction with the adult age group (35-54 yo), with OR for dysthymic males ranging from 8.3 to 14.9. Female gender was not associated with “suicide attempt”. None of the two- or three-way interaction effects tested was significant for “suicide attempt”.
We also tested the effect of association between DSM-III-R non-affective psychosis and SCB (data not shown). It presented an association only in model 1 for “thoughts of death” (OR = 2.5; 95% CI 1.1-5.7) and “suicidal thoughts” (OR = 3.1; 95% CI 1.2-7.8). For “thoughts of death”, females presented OR = 1.6 (95% CI 1.2-2.0) and a protective effect for those previously married (OR = 0.5; 95% CI 0.3-0.8). Other models and other SBC could not be calculated due to the small sample size of psychotic individuals (N = 7).
Discussion
Our results showed that, in the present community sample, depressive disorders are important predictors of suicide-related cognitions and behaviors, independently of the presence of AUD/SUD, gender or other demographic correlates. However, the totality of SCB was liable to be influenced by a variety of effects of depressive disorders and AUD/SUD, either independently or as comorbid diagnoses. Even though the odds of two broad classes of internalizing and externalizing disorders with SCB are significant from the bivariate perspective, the multivariate regression analysis showed a complex and interconnected relationship of this frequent clinical phenomenology of suicidal individuals, thus demonstrating the differential effects of these frequently occurring comorbid disorders in SCB. Accordingly, this study underscores the importance of assessing the comorbidity of internalizing depressive disorders and externalizing AUD/SUD in suicide-prone individuals.
With regard to socio-demographic variables, generally females reported higher rates of SCB than males, as found in previous studies.2,9,31,32 Furthermore, in MDE models, female gender was associated only with “thoughts of death”. On the other hand, in models for dysthymia, female gender was associated with all SCB except “suicide attempt”. Regarding this specific SCB, both in the MDE and in the dysthymia models the age subgroup from 35 to 54 year old. males was associated with “suicide attempts” while female gender was not associated with such SBC; data not supported by some studies.32-35 For “thoughts of death”, the effect of female gender remained significant even after controlling for AUD/SUD.9,32 In other SCB, the influence of female gender in suicidality varied according to the disorders considered. Even though there were no gender differences in the frequency of “suicidal thoughts” as assessed in our study, we observed an interactive effect of gender, where dysthymic males were approximately five times more likely than dysthymic females to report such suicidal cognition even in the presence of AUD. Possibly, this gender difference in suicidality might be accounted for by the effect of externalizing and internalizing liability factors encountered in men and women, arising from neurobiological diversity and the effects of genetic and environmental risk factors,22 resulting in different prevalence in broad spectra of internalizing-externalizing disorders.36 Other socio-demographic variables involved in SCB were marital status and educational level. The disadvantaged poorly-educated (i.e. with an educational level less than “some form of higher education”) and the lack of an interpersonal relationship (never married or previously married people) were associated with a higher risk for some SCB.31,32,37 Our empirical data suggest that different types of predictors might exert an influence across all stages of progression of SCB along the suicidal continuum.4
The phenomenon of comorbidity can be alternatively described as a multimorbidity phenomenon, since patterns of association among mental disorders involve multiple disorders across the nosological system.38 Flexible multivariate models of comorbidity should be investigated to achieve a parsimonious solution to describe what happens in the real world. Rather than discussing theoretical concepts or classifying psychopathologies, our focus is to depict how the presence of distinct externalizing-internalizing psychopathologies could putatively lead to changes in severity among suicidal individuals. First, comparing bivariate and multivariate regression of the psychiatric disorders on SCB, it is clear that the co-occurrence of both disorders accounted in different ways for most of the data variance. Nevertheless, depressive disorders seemed to play a more notable role in generating suicidal cognitions and behavior than did AUD/SUD.31,34 In a recent European study, some socio-demographic variables and psychiatric diagnoses were found to be related to suicidality, and major depressive disorder was found with the higher population attributable risk among the assessed predictors of SCB (“suicidal thoughts” and “suicide attempts”).32 Unfortunately, the effect of the comorbid internalizing and externalizing disorders was not tested in relation to the SCB.
A strength of our comorbidity models was to take into account the pattern of interaction between independent diagnoses and SCB, as well as some demographic variables. By using an analytic strategy of correlated data approach (GEE), the robustness of the results found should be underscored. In a hazardous analysis of the effect of psychiatric disorders and SCB among adolescents, the interactive effect of mood disorders and AUD increased the risk for attempted suicide.34 When lifetime psychiatric comorbidities were controlled, the strength of association between SCB and SUD was smaller than in uncontrolled analysis, while still associated.31 Indeed, there was a heterogeneity effect for co-occurring dysthymia and gender and this effect remains even in the presence of AUD/SUD.9,32
Major depressive episode and dysthymia remained significantly associated with all SCB for each multivariate model we tested. When compared to patients with episodic major depressive disorder in a clinical setting, dysthymic patients presented more propensities to have a history of AUD/SUD, a more stable psychopathology, and severe global impairment.39-41 In a follow-up study of AUD and SUD patients, major depressive disorder and dysthymia were associated with lifetime “suicide attempt” at admission, but only dysthymia remained associated with increased risk of suicide attempt during the follow-up.37
Despite dysthymia being generally viewed as a persistent and milder form of major depressive disorder, its clinical effects on SCB might be overlooked39,42 as it might be consistently associated with SBC, specially in men. At first, the proportion of “suicide attempts” was found to be significantly greater among patients with early-onset dysthymia than those with episodic major depressive disorder.39 The presence of cognitive symptoms prevails over vegetative and psychomotor symptoms in individuals with the diagnosis of dysthymia.43 Additionally, the presence of rumination has been associated with an increase in thoughts of suicide.44 Previous data from a 20-year prospective study indicate that chronic psychiatric disorders may play a relevant role for suicide risk, since a diagnosis of recurrent major depressive disorder was a significant risk factor, while a single episode of major depressive disorder was not.45 Thinking about death and suicide would represent a strategy to deal with or stop an unbearable aversive situation, especially if that situation persists over the long term.35,44 Possible explanations for such a role for dysthymia in SCB involve looking at its core symptoms that can impair the coping strategies.35
AUD appeared consistently as an important independent risk factor for all SCB and could predict their occurrence even when controlled for MDE, dysthymia and gender.12,31,46,47 It also presented an interaction with MDE in “thoughts of death”. In that case, individuals presenting with MDE or AUD are associated with SCB, while those who presented with comorbid MDE and AUD are not associated with this SBC. However, when SUD were added to the models, part of the association of depressive disorders with SCB was dispersed in the case of substance disorders, as SUD was no longer associated with SCB in most of the models.45 Disorders characterized by poor impulse control, such as SUD, are especially useful in the prediction of unplanned suicide attempts.4,31 Accordingly, the use of alcoholic beverages could also possibly trigger impulsive suicidal attempts.34 It seems that the type of disorder predicts differently the outcome of non-fatal suicide attempt.4
The interpretation of the findings of this present study on SCB involving comorbid depressive disorders, non-affective psychosis and AUD/SUD should be viewed bearing in mind some limitations. First, there could have been an information bias that emerged from the sort of interview we adopted – a household face-to-face interview – which in general would select individuals presenting less severe psychopathology. Since alcohol use, substance use, and SCB were not socially desirable behaviors in some social strata and information was conditioned to retrospective reports, an unwillingness to cooperate, and recall bias, might affect the reliability of data. Second, individuals presenting a diagnosis of alcohol or substance use disorder (abuse or dependence) account for only 5.5% and 1.1% of the sample, respectively.23 In a recent nationwide Brazilian household survey48 higher rates of alcohol and substance consumption were observed. The lifetime prevalence of alcohol use was 11.2%, and lifetime prevalence of substance use ranged from 6.9% for cannabis to 0.1% for heroin. For instance, our statistical strategy and the low prevalence of SUD might have increased the possibility of type II error, i.e. lack of association between SUD and SCB. Third, several disorders identified as associated with SCB, such as panic disorder and personality disorders, were not examined in this study, remaining an issue for future researches. Although DSM-III-R non-affective psychosis was also examined, most regression analysis could not be performed due to the small sample size. Finally, in a lifetime prevalence study with a mixed-age sample data can create the appearance of comorbidity, or pseudo-comorbidity, even when disorders are randomly associated.49 In the present study, we were unable to evaluate differences in present and past use of substances for lifetime prevalence, or at which phase of use the subjects were (withdrawal, remission, or presently using).
Conclusion
The presence of depressive disorders is an important predictor for nonfatal suicide-related cognitions and behaviors. Nevertheless, the presence of AUD/SUD can increase the risk of suicide in some groups of individuals. The clinical implication of these findings is to stress the importance of the routine assessment of comorbid psychiatric disorders, particularly substance and alcohol use disorders, when managing risk in suicidal patients. The findings have decisive implications in the clinical strategies of reducing suicidality.
In the future, large sample population studies should observe in detail the complex psychopathology of suicidal behaviors and the correlations with externalizing-internalizing disorders. Conducting a prospective longitudinal design of study would confirm the role of hypothetical risk factors; and ascertaining the phase of substance use would avoid some data collection bias. Powerful multivariate model-based analysis such as confirmatory factor analysis, latent class analysis, or more general mixture models should be adopted to depict underlying latent variables of the phenomenon of comorbidity. In future, it should be the task of researchers on suicidology to take into account the mechanisms through which the comorbidity pattern can lead to suicide, contributing to the establishment of a model to explain these SCB.

References
1. Arsenault-Lapierre G, Kim C, Turecki G. Psychiatric diagnosis in 3275 suicides: a meta-analysis. BMC Psychiatry. 2004;4:37. [ Links ]
2. Harris EC, Barraclough B. Suicide as an outcome for mental disorders: a meta-analysis. Br J Psychiatry. 1997;170(3):205-28. [ Links ]
3. Brown GK, Steer RA, Henriques GR, Beck AT. The internal struggle between the wish to die and the wish to live: a risk factor for suicide. J Consult Clin Psychol. 2005;162(10):1977-9. [ Links ]
4. Nock MK, Hwang I, Sampson N, Kessler RC, Angermeyer M, Beautrais A, Borges G, Bromet E, Bruffaerts R, de Girolamo G, de Graaf R, Florescu S, Gureje O, Haro JM, Hu C, Huang Y, Karam EG, Kawakami N, Kovess V, Levinson D, Posada-Villa J, Sagar R, Tomov T, Viana MC, Williams DR. Cross-national analysis of the associations among mental disorders and suicidal behavior: findings from the WHO World Mental Health Surveys. PLoS Med. 2009;6(8):e1000123. [ Links ]
5. Mościcki EK. Identification of suicide risk factors using epidemiologic studies. Psychiatr Clin North Am.1997;20(3):499-517.
6. Sher L. Alcoholism and suicidal behavior: a clinical overview. Acta Psychiatr Scand. 2006;113(1):13-22. [ Links ]
7. Menezes PR, Mann AH. Mortality among patients with non-affectivefunctional psychoses in a metropolitan area of South-Eastern Brazil. Rev Saude Publica. 1996;30(4):304-9. [ Links ]
8. Limosin F, Loze JY, Philippe A, Casadebaig F, Rouillon F. Ten-year prospective follow-up study of the mortality by suicide in schizophrenic patients. Schizophr Res. 2007;94:23-8. [ Links ]
9. Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):
617-27.
10. Krueger RF, Markon KE. Reinterpreting comorbidity: a model-based approach to understanding and classifying psychopathology. Annu Rev Clin Psychol. 2006;2:111-33. [ Links ]
11. Melartin TK, Rytsälä HJ, Leskelä US, Lestelä-Mielonen PS, Sokero TP, Isometsä ET. Current comorbidity of psychiatric disorders among DSM-IV major depressive disorder patients in psychiatric care in the Vantaa Depression Study. J Clin Psychiatry. 2002;63(2):126-34. [ Links ]
12. Sher L, Oquendo MA, Galfalvy HC, Grunebaum MF, Burke AK, Zalsman G, Mann J. The relationship of aggression to suicidal behavior in depressed patients with a history of alcoholism. Addict Behav. 2005;30(6):1144-53. [ Links ]
13. Sher L, Stanley BH, Harkavy-Friedman JM, Carballo JJ, Arendt M, Brent DA, Sperling D, Lizardi D, Mann JJ, Oquendo MA. Depressive patients with co-ocurring alcohol use disorders: a unique patient population. J Clin Psychiatry. 2008;69(6):907-15. [ Links ]
14. Regier DA, Farmer ME, Rae DS, Locke BZ, Keith SJ, Judd LL, Goodwin FK. Comorbidity of mental disorders with alcohol and other drug abuse. Results from the Epidemiologic Catchment Area (ECA) Study. JAMA. 1990;264(19):2511-8. [ Links ]
15. Merikangas KR, Angst J, Eaton W, Canino G, Rubio-Stipec M, Wacker H, Wittchen HU, Andrade L, Essau C, Whitaker A, Kraemer H, Robins LN, Kupfer DJ. Comorbidity and boundaries of affective disorders with anxiety disorders and substance misuse: results of an international task force. Br J Psychiatry. 1996;168(Suppl 30):58-67. [ Links ]
16. Kessler RC, Aguilar-Gaxiola S, Andrade L, Bijl R, Borges G, Caraveo-Anduaga JJ, DeWit DJ, Kolody B, Merikangas KR, Molnar BE, Veja WA, Walters EE, Wittchen HU, Ustun TB. Mental-substance comorbidities in the ICPE surveys. Psychiatria Fennica. 2001;32(Suppl 2):62-80. [ Links ]
17. Conway KP, Compton W, Stinson FS, Grant BF. Lifetime comorbidity of DSM-IV mood and anxiety disorders and specific drug use disorders: results from the National Epidemiologic Survey on Alcohol and Related Conditions. J Clin Psychiatry. 2006;67(2):247-57. [ Links ]
18. Wilcox HC, Conner KR, Caine ED. Association of alcohol and drug use disorders and completed suicide: an empirical review of cohort studies. Drug Alcohol Depend. 2004;76(Suppl 1):S11-9. [ Links ]
19. Mann JJ, Oquendo M, Underwood MD, Arango V. The neurobiology of suicide risk: a review for the clinician.J Clin Psychiatry. 1999;60(Suppl 2):7-11. [ Links ]
20. Wassermann D. Suicide: an unnecessary death. London UK: Martin Dunitz; 2001. [ Links ]
21. Kessler RC. The epidemiology of dual diagnosis. Biol Psychiatry. 2004;56(10):730-7. [ Links ]
22. Kendler KS, Jacobson KC, Prescott CA, Neale MC. Specificity of genetic and environmental risk factors for use and abuse/dependence of cannabis, cocaine, hallucinogens, sedatives, stimulants, and opiates in male twins. Am J Psychiatry. 2003;160(4):687-95. [ Links ]
23. Andrade LH, Walters EE, Laurenti R, Gentil V. Prevalence of ICD-10 mental disorders in a catchment area in the city of São Paulo, Brazil. Soc Psychiatry Psychiatr Epidemiol. 2002;37(7):316-25. [ Links ]
24. Fundação IBGE – Instituto Brasileiro de Geografia e Estatística. Pesquisa nacional por amostra de domicílios: resultados do censo de população. São Paulo: Tabulação especial; 1995. [ Links ]
25. Kish L. Survey sampling. John Wiley and Sons Inc: New York; 1965. [ Links ]
26. Miranda CT, Mari JJ, Ricciardi A, Arruda ME. Patients’ reactions to the CIDI in Brazil. In: Stefanis CN, Rabavillas AD, Soldatos CR, editors. Psychiatry: a world in perspective. Amsterdam, the Netherlands: Elsevier; 1990. [ Links ]
27. Wittchen HU, Robins LN, Cottler LB, Sartorius N, Burke JD, Regier D. Cross-cultural feasibility, reliability and sources of variance of the Composite International Diagnostic Interview (CIDI). The Multicentre WHO/ADAMHA Field Trials. Br J Psychiatry. 1991;159:645-53, 658. [ Links ]
28. Liang KY, Zeger SL. Longitudinal data analysis using generalized linear models. Biometrika. 1986;73:13-22. [ Links ]
29. Zeger SL, Liang KY, Albert PS. Models of longitudinal data: a generalized linear equation approach.Biometrics. 1988;77:642-8. [ Links ]
30. SAS – Statistical Analysis System. User’s guide. Cary (NC): SAS Institute; 1996. [ Links ]
31. Borges G, Walters EE, Kessler RC. Associations of substance use, abuse, and dependence with subsequence suicidal behavior. Am J Epidemiol. 2000;151(8):781-90. [ Links ]
32. Bernal M, Haro JM, Bernert S, Brugha T, de Graaf R, Bruffaerts R, Lépine JP, de Girolamo G, Vilagut G, Gasquet I, Torres JV, Kovess V, Heider D, Neeleman J, Kessler R, Alonso J, the ESEMED/MHEDEA Investigators. Risk factors for suicidality in Europe: Results from the ESEMED study. J Affect Disord. 2007;101(1-3):27-34. [ Links ]
33. Bolton JM, Belik SL, Enns MW, Cox BJ, Sareen J. Exploring the correlates of suicide attempts among individuals with major depressive disorder: findings from the national epidemiologic survey on alcohol and related conditions. J Clin Psychiatry. 2008;69(7):1139-49. [ Links ]
34. Kelly TM, Cornelius JR, Clark DB. Psychiatric disorders and attempted suicide among adolescents with substance use disorders. Drug Alcohol Depend. 2004;73(1):87-97. [ Links ]
35. Barnow S, Linden M. Epidemiology and psychiatric morbidity of suicidal ideation among the elderly. Crisis. 2000;21(4):171-80. [ Links ]
36. Kramer MD, Krueger RF, Hicks BM. The role of internalizing and externalizing liability factors in accounting for gender differences in the prevalence of common psychopathological syndromes. Psychol Med. 2008;38(1):51-61. [ Links ]
37. Bakken K, Vaglum P. Predictors of suicide attempters in substance-dependent patients: a six-year prospective follow-up. Clin Pract Epidemol Ment Health. 2007;3:20. [ Links ]
38. Batstra L, Bos EH, Neeleman J. Quantifying psychiatric comorbidity: lessons from chronic disease epidemiology. Soc Psychiatry Psychiatr Epidemiol. 2002;37(3):105-11. [ Links ]
39. Klein DN, Norden KA, Ferro T, Leader JB, Kasch KL, Klein LM, Schwartz JE, Aronson TA. Thirty-month naturalistic follow-up study of early-onset dysthymic disorder: course, diagnostic stability, and prediction of outcome. J Abnorm Psychol. 1988;107(2):338-48. [ Links ]
40. Klein DN, Taylor EB, Dickstein S, Harding K. Primary early-onset dysthymia: comparison with primary nonbipolar nonchronic major depression on demographic, clinical, familial, personality, and socioenvironmental characteristics and short-term outcome. J Abnorm Psychol. 1988;97(4):387-98. [ Links ]
41. Klein DN, Shankman SA, Rose S. Ten-year prospective follow-up study of the naturalistic course of dysthymic disorder and double depression. Am J Psychiatry. 2006;163(5):872-80. [ Links ]
42. Klein DN, Schwartz JE, Rose S, Leader JB. Five-year course and outcome of dysthymic disorder: a prospective, naturalistic follow-up study. Am J Psychiatry. 2000;157(6):931-9. [ Links ]
43. Serretti A, Jori MC, Casadei G, Ravizza L, Smeraldi E, Akiskal H. Delineating psychopathologic clusters within dysthymia: a study of 512 out-patients without major depression. J Affect Disord. 1999;56(1):17-25. [ Links ]
44. Miranda R, Nolen-Hoeksema S. Brooding and reflection: Rumination predicts suicidal ideation at 1-year follow-up in a community sample. Behav Res Ther. 2007;45(12):3088-95. [ Links ]
45. Brown GK, Beck AT, Steer RA, Grisham JR. Risk factors for suicide in psychiatric outpatients: a 20-year prospective study. J Consult Clin Psychol. 2000;68(3):371-7. [ Links ]
46. Preuss UW, Schuckit MA, Smith TL, Danko GP, Bucholz KK, Hesselbrock MN, Hesselbrock V, Kramer JR. Predictors and correlates of suicide attempts over 5 years in 1,237 alcohol-dependent men and women. Am J Psychiatry. 2003;160(1):56-63. [ Links ]
47. Cottler LB, Campbell W, Krishna VAS, Cunningham-Williams RM, Abdallah AB. Predictors of high rates of suicidal ideation among drug users. J Nerv Ment Dis. 2005;193(7):431-7. [ Links ]
48. Carlini EA, Galduróz JCF, Noto AR, Nappo SA. Levantamento domiciliar sobre o uso de drogas psicotrópicas no Brasil: Estudo envolvendo as 107 maiores cidades do país – 2001. São Paulo: Centro Brasileiro de Informações Sobre Drogas Psicotrópicas – CEBRID – Universidade Federal de São Paulo – UNIFESP; 2002. [ Links ]
49. Kraemer HC, Wilson KA, Hayward C. Lifetime prevalence and pseudocomorbidity in psychiatric research.Arch Gen Psychiatry. 2006;63(6):604-8. [ Links ]
Correspondence
Bruno Mendonça Coêlho
Núcleo de Epidemiologia Psiquiátrica
Instituto de Psiquiatria do Hospital das Clínicas
Faculdade de Medicina da Universidade de São Paulo
Rua Dr. Ovídio Pires de Campos, 785
05403-010 São Paulo, SP, Brazil
Phone/Fax: (+ 55 11) 3069-6976
Email: brunomendoncacoelho@yahoo.com.br
Submitted: July 23, 2009
Accepted: April 27, 2010
* Parts of the present article were presented during the World Psychiatric Association Meeting in Prague, Czech Republic, September 2008. It also received the “Sergio De Risio Award” at the same meeting.