Intimate partner violence trends in Brazil: data from two waves of the Brazilian National Alcohol and Drugs Survey
Revista Brasileira de Psiquiatria
Print version ISSN 1516-4446
On-line version ISSN 1809-452X
Rev. Bras. Psiquiatr. vol.38 no.2 São Paulo Apr./June 2016
http://dx.doi.org/10.1590/1516-4446-2015-1798
Original Articles
Intimate partner violence trends in Brazil: data from two waves of the Brazilian National Alcohol and Drugs Survey
1Instituto Nacional de Ciência e Tecnologia para Políticas Públicas do Álcool e Outras Drogas (INPAD), Departamento de Psiquiatria, Universidade Federal de São Paulo (UNIFESP), São Paulo, SP, Brazil
2Universidade Federal do Espírito Santo (UFES), Vitoria, ES, Brazil
3Prevention Research Center, Pacific Institute for Research and Evaluation, Calverton, MD, USA
Objective:
To compare intimate partner violence (IPV) prevalence rates in 2006 and 2012 in a nationally representative household sample in Brazil. The associations between IPV and substance use were also investigated.
Methods:
IPV was assessed using the Conflict Tactic Scale-R in two waves (2006/2012) of the Brazilian Alcohol and Drugs Survey. Weighted prevalence rates and adjusted logistic regression models were calculated.
Results:
Prevalence rates of IPV victimization decreased significantly, especially among women (8.8 to 6.3%). The rates of IPV perpetration also decreased significantly (10.6 to 8.4% for the overall sample and 9.2 to 6.1% in men), as well as the rates of bidirectional violence (by individuals who were simultaneously victims and perpetrators of violence) (3.2 to 2.4% for the overall sample). Alcohol increased the likelihood of being a victim (odds ratio [OR] = 1.6) and perpetrator (OR = 2.4) of IPV. Use of illicit drugs increased up to 4.5 times the likelihood of being a perpetrator.
Conclusions:
In spite of the significant reduction in most types of IPV between 2006 and 2012, violence perpetrated by women was not significantly reduced, and the current national rates are still high. Further, this study suggests that use of alcohol and other psychoactive drugs plays a major role in IPV. Prevention initiatives must take drug misuse into consideration.
Key words: Domestic violence; intimate partner violence; epidemiology; violence; Brazil
Introduction
Intimate partner violence (IPV) is an important public health problem. According to the World Health Organization (WHO), the global lifetime prevalence of IPV among ever-partnered women is about 30%, ranging from 20 to 40% for different regions around of world. Compared to men victimized by IPV, women are more likely to have serious injuries.1 2–3 Of importance, more than one in 10 homicides is perpetrated by an intimate partner, and more than a third of female homicides are perpetrated by partners.1
Even though several studies have shown higher prevalence rates of domestic violence among Latino populations as compared to other ethnic groups,4,5 only scarce data on the subject are available in Latin America4,6,7. According to a recent WHO report, Brazil ranks seventh in female homicide rates among 84 countries of the world, surpassing most of its South American neighbors except Colombia, all European countries except Russia, and all African and Arabic countries.7,8 A 2012 national survey conducted by the Brazilian government revealed that over 18% of the national female population reported having been a victim of IPV.9 Over half of Brazilian men reported having performed at least one violent act against their partners, although only 16% viewed their behavior as violent.10 Finally, data from a survey conducted in the largest cities in Brazil revealed that 8.6% of the sample reported being victims of intimate partner sexual violence, mostly women.11 In the first Brazilian Alcohol and Drugs Survey (I BNADS), performed in 2006, IPV was reported by over 10% of the men and by 15% of the women from a nationally representative sample.12
To address the high rates of violence against women in Brazil, a new law providing measures to control gender violence against women was enacted in 2006. This law, identified by the name of an IPV victim, Maria da Penha, introduced more stringent criminal treatment for violence against women13 as well as conceptual innovations, such as the recognition of different forms of violence (physical, psychological, sexual, property-related, and moral).10 The new legislation was put in place in 2006, concomitantly with the first wave of the I BNADS. The II BNADS was performed 6 years after the implementation of the Maria da Penha Law, providing an opportunity to assess trends in IPV in the country before and after the law was implemented.
The associations between domestic violence (IPV and/or childhood abuse) and several factors have been largely studied.14 15–16 There is consistent evidence showing higher rates of IPV among heavy drinkers and alcohol dependents. The I BNADS confirmed the association between IPV and alcohol consumption.12 The use of other substances, such as multiple drugs, tobacco, and hypnotics, is also frequently associated with IPV.17
The aim of the present study was to examine IPV trends in Brazil, as well as to investigate the sociodemographic predictors of IPV victimization and perpetration and possible associations of IPV with alcohol, tobacco, and illegal substances.
Methods
This is a cross-sectional study based on the two waves of the BNADS. Comparative analysis was performed using both datasets (2006/2012), whilst associations were investigated using data from the 2012 wave only.
Sampling and procedures (2006 and 2012 surveys)
Both surveys were organized by the National Institute of Alcohol and Drugs Policy (Unidade de Pesquisa em Álcool e Drogas, INPAD) of Universidade Federal de São Paulo, Brazil, and conducted by Ipsos Public Affairs. Both surveys used multistage cluster sampling to select Brazilians 14 years of age and older from the country’s household population. In both surveys, face-to-face interviews of about one hour were carried out by trained interviewers. Sampling methods were identical in both surveys. Multistage sampling had four stages, as follows: counties, within counties census areas, households, and, at the last stage, a randomly selected respondent within the household. No substitutions were allowed. In 2006, the selected sample was composed of 3,007 participants, comprised by 2,346 interviews with adults (≥18 years of age) plus 661 with respondents between 14 and 17 years of age. In 2012, 4,607 participants were interviewed, including 3,295 respondents ≥ 18 years of age and 1,312 respondents between 14 and 17 years of age. The response rate in 2006 was 66%, vs. 77% in 2012. A subsample of 1,443 (55.34%) participants in 2006 and 2,120 (57.18%) in 2012, all of whom were either married or living with a partner was used for analysis in the present study.
Measurements
Sociodemographic variables
In this analysis, all the main sociodemographic variables were assessed – gender, age, education, socioeconomic status, income, and all the Brazilian geographic regions: North, Northeast, Midwest, Southeast, and South.
Intimate partner violence
All questions regarding physical violence were adapted from The Revised Conflict Tactics Scales (CTS2).18 Respondents were asked nine questions about the occurrence of different types of violent behaviors in the last 12 months, including minor violence (throwing something, pushing, grabbing, shoving, slapping) and severe violence (kicking, biting, or hitting, hitting or trying to hit with something, burning or scalding, forced sex, threatening with a knife or gun, using a knife or gun). First, respondents were asked if they had perpetrated these acts against their partner and then were asked to report if their partner had perpetrated these acts against them. Based on their responses, a five-level variable was created (none, 1, 2, 3, or more events). A binary variable was also created combining the events, where 1 was attributed to individuals who were positive (as victims or perpetrators) to at least one event.
Substance use
Alcohol consumption: binge drinking
Determined according to the National Institute on Alcohol Abuse as consuming five or more units/drinks for men or four for women in about 2 h. Occurrence in the previous year was considered as positive.
Alcohol consumption: DSM-5 alcohol use disorders (AUD)
Assessed with the Brazilian version of the Composite International Diagnostic Interview.19 Although this interview pre-dates DSM-5, it has a question about craving, which allowed for the creation of a diagnosis that followed DSM-5 criteria in full. All 11 criteria in the DSM-5 were covered. A cutoff point of two or more criteria present in the past 12 months was adopted for a positive diagnosis of AUD.
Tobacco use
Participants were asked about their consumption of tobacco products (cigarettes, roll-ups, pipes, or cigars) and about their patterns of consumption (amount consumed, frequency of use in the last 30 days).
Sedative use
Respondents were asked about the use of diazepam, bromazepam, and clonazepam daily and in the preceding 12 months.
Illicit drug use
Defined as lifetime or 12-month self-reported use of the following substances: cannabis, amphetamine type stimulants (such as speed, crystal meth, ecstasy, and other MDMA alternatives), crack/cocaine, cocaine and other illegal drugs (solvents, glue, and ether-chloride spray), opioids (heroin and morphine), and hallucinogens (LSD, magic mushrooms).
Illicit drug use and sedative use assessments were modified in the 2012 wave. To guarantee confidentiality, those questions were not asked face-to-face anymore, but completed separately by the participant and returned in sealed envelopes to the interviewer. This change prevents a comparison between the two waves for these variables. Therefore, associations between IPV and illicit drug use were only investigated for the second wave of the survey.
Survey wave
A binary variable was created to indicate the survey year (2006 or 2012). The merged dataset was used to compare the sociodemographic characteristics and AUD associations with IPV.
Statistical analysis
Statistical analyses were conducted using STATA v.13.0. All analyses were weighted to take into account the multistage design of the sample and of non-response using post-stratification. All estimates of prevalence rates and regression models were made using the STATA survey commands (svy) to generate robust standard errors. The first stage of analysis was performed using a merged dataset where survey waves 2006/2012 were combined. Sociodemographic characteristics are described in the married and cohabiting population and among those involved in domestic violence considering three categories: those who reported being a victim, those who reported being a perpetrator, and those who belonged to both groups and were considered the “bidirectional” group. All prevalence rates were compared between the waves using the chi-square test (p < 0.05). The second stage of analysis was performed using the second wave of the survey alone. Stepwise multivariate logistic regression models were carried out to test associations between the three categories of IPV (victims/perpetrators/bidirectional) and sociodemographic characteristics and substance use (alcohol, tobacco, and illegal drug use). All models were mutually adjusted, and associations with use of alcohol and other substances were controlled by sociodemographic characteristics.
Results
Sample characteristics
All analyses for this study were performed with married/cohabiting participants, equivalent to 55.3% of the total sample in 2006 and 57.2% of the 2012 wave. Both samples were almost equally distributed between genders and weighted by education and socioeconomic status.
IPV trends between 2006 and 2012
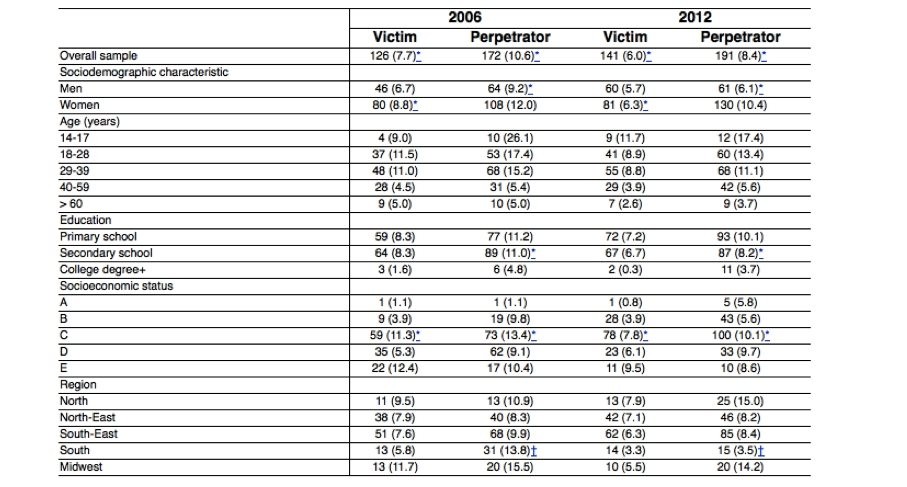
A significant decrease in IPV victimization was observed between 2006 and 2012, mostly in women (8.8% in 2006 and 6.3% in 2012). The odds of IPV victimization significantly decreased in 2012 (odds ratio [OR] = 0.73, 95% confidence interval [95%CI] 0.55-0.95 – adjusted by sex, age, education, and income). Even though no differences were detected in these rates in men, the reduction was significant for the overall population (7.7% in 2006 to 6% in 2012). Regarding socioeconomic status, only class C had significant reductions in IPV victimization (11.3% in 2006 to 7.8% in 2012) (Table 1).
Table 1 Prevalence rates of victimization and perpetration of at least one event of violence between 2006 and 2012 by sociodemographic characteristics
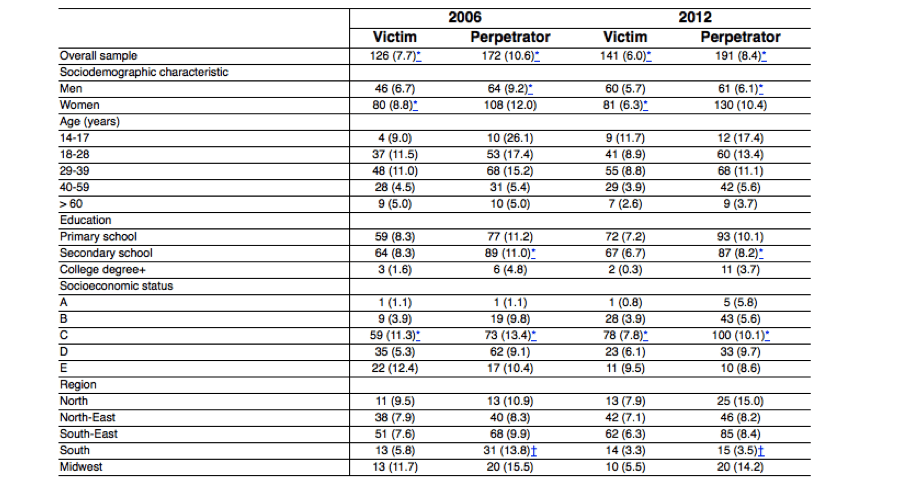
Data presented as n (%).
All prevalence rates calculated by row.
*Indicates significance (p < 0.05) in chi-square test to verify differences between the two waves.
†p < 0.01.
Nearly 1 in 10 Brazilians (8.4%) reported being a perpetrator of inter-partner violence in 2012 (Table 1). In 2006, over 1 in 10 participants referred having displayed at least one type of aggressive behavior against their partners (10.6%). The chances of displaying an aggressive behavior significantly decreased between the two waves (OR = 0.68, 95%CI 0.54-0.86). There was a small difference between males and females, with women reporting higher rates of perpetration of violence compared to men (12% women and 9.2% men). The reduction between the two waves was significant among men (9.2 to 6.1%), among participants from the lower middle class (13.4 to 10.1%), and among those with secondary school diploma (11.0 to 8.2%). Regarding Brazilian regions, significant reduction was only observed in the South, from 13.8% in 2006 to 3.5% in 2012 (Table 1).
The rate of participants who referred being both victims and perpetrators of intimate violence decreased significantly between the two waves (3.2% in 2006 vs. 2.4% in 2012) (Table 2).
Table 2 Prevalence rates of intimate partner violence across genders in 2006 and 2012
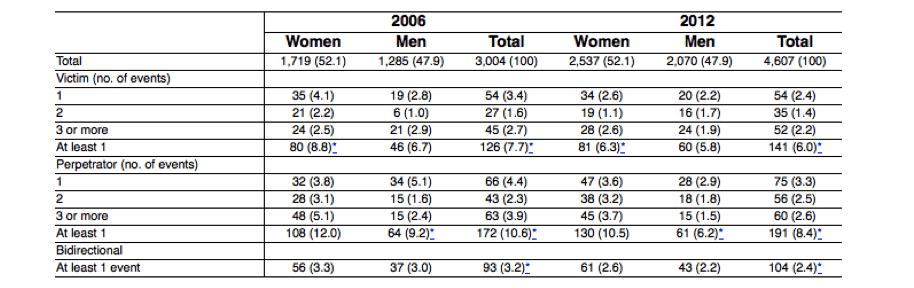
Data presented as n (%).
*p < 0.05 chi-square to test differences between the two waves.
Associations between IPV and sociodemographic characteristics
In men, education was a protective factor against aggression (complete primary school and complete secondary school vs. illiterate or incomplete primary school) (OR = 0.22, 95%CI 0.06-0.79, p < 0.05; OR = 0.18, 95%CI 0.04-0.83, p < 0.05 respectively). Older age was a protective factor for perpetration of violence in both men (incidence rate ratio [IRR]: 0.97, 95%CI 0.95-0.99, p < 0.05) and women (IRR: 0.97, 95%CI 0.95-0.98, p < 0.001) (result not shown in tables). In other words, older or more educated males were less likely to perpetrate violence than younger or less educated men. Older females were less likely to perpetrate violence against their partners. Gender and socioeconomic status were not significantly associated with victimization or perpetration of IPV.
IPV and substance use
Victimization
Regarding substance consumption, it was found that nearly one third of the overall population referred binge drinking and 10% were alcohol dependents (results not shown in tables) in 2012. In women, we found no associations between being a victim of IPV and substance consumption. None of the substances studied except alcohol were associated with being a victim of IPV. A significant association between men victims of IPV and DSM-5 AUD was identified. Men IPV victimization was also associated with binge drinking (OR = 3.88, 95%CI 1.65-9.16 for dependence and OR = 2.37, 95%CI 1.15-4.92 for binge). The associations between IPV victimization and the alcohol misuse variables (AUD and binge) were also significant when considering the overall sample (OR = 2.52, 95%CI 1.36-4.66 for AUD) in 2012 (Table 3) and remained significant in the analysis of the merged dataset of 2006 and 2012 survey waves combined (OR = 4.15, 95%CI 3.21-5.36 for AUD and OR = 1.99, 95%CI 1.55-2.54 for binge drinking) and when adjusted by survey wave (OR = 4.11, 95%CI 3.18-5.31 for AUD and OR = 2.03, 95%CI 1.59-2.61 for binge drinking).
Table 3 Substance use prevalence rates and associations with intimate partner violence in victims, perpetrators, and victims/perpetrators (bidirectional violence)
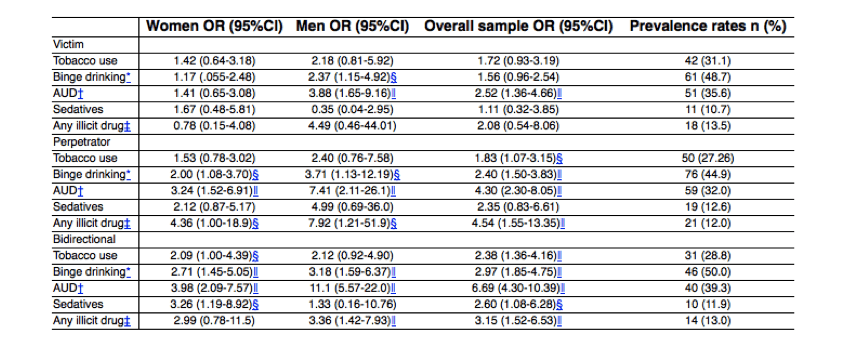
All regression models were controlled by age, education, and income (sex for overall sample). Victimization models were controlled by perpetration and vice-versa.
95%CI = 95% confidence interval; AUD = alcohol use disorders; OR = odds ratio.
*Previous year ingestion of 4 (women) and 5 (men) or more units of alcohol within 2 h.
†According to DSM-5 criteria.
‡Use of any illicit substance in the previous year.
§p < 0.05 (logistic regression).
‖p < 0.01 (logistic regression).
Perpetration
Nearly 45% of the participants who referred being an IPV perpetrator were binge drinkers: 32% were identified with AUD (Table 3) – compared to 27 and 10% respectively in the overall population. Being a perpetrator of violence was associated with binge drinking in the overall sample (OR = 2.40, 95%CI 1.50-3.83) and AUD (OR = 4.30, 95%CI 2.30-8.05). This association was even stronger among male perpetrators, who were nearly four times more likely to binge drink (OR = 3.71, 95%CI 1.13-12.19) and over seven times more likely to be alcohol dependents (OR = 7.41, 95%CI 2.11-26.1) (Table 3). We also found that nearly a third of the aggressors were smokers (Table 3), with a significant association between smoking and IPV for the overall sample. Also, more than 1 in 10 perpetrators of violence had used at least one illicit drug in the previous year (Table 3). The use of illegal drugs was highly associated with IPV (OR = 4.54, 95%CI 1.55-13.35 for whole sample). This association was significant for both genders, especially men (OR = 7.92, 95%CI 1.21-51.9).
Bidirectional IPV
The prevalence rates of substance use among individuals who reported bidirectional IPV (being both a victim and a perpetrator of IPV) were significantly higher. Nearly one third of the individuals in this group were smokers, half referred binge drinking, nearly 40% referred AUD, and 13% referred illegal drug use (Table 3).
Mutual violence more than doubled the likelihood of binge drinking and being alcohol dependent in men and women (OR = 2.71, 95%CI 1.45-0.05 for females and OR = 3.18, 95%CI 1.59-6.37 for males for binge drinking; and OR = 3.98, 95%CI 2.09-7.57 for women and OR = 11.1, 95%CI 5.57-22.01 for men for AUD). Illegal drug use was also highly associated with bidirectional IPV in men (OR = 3.36, 95%CI 1.42-7.93), but not in women. Sedative use was significantly associated with bidirectional violence in women (OR = 3.26, 95%CI 1.19-8.92) (Table 3).
Discussion
The BNADS, conducted in 2006 and 2012, interviewed a nationally representative household sample, generating comparable data from the period before and after a major change in legislation tackling IPV. The findings presented here highlight that a meaningful proportion of Brazilians of all ages and different sociodemographic status still experience IPV, even though a decrease was observed for some of the rates. More than 10% of married/cohabiting Brazilians perpetrated at least one form of IPV in 2006, compared to just over 8% in 2012, indicating a significant reduction in this 6-year period, especially for men. The same was detected for IPV victims in the two waves, with a significant reduction from 7.8% in 2006 to 6% in 2012. This decrease was even more marked for women who suffered at least one type of violence, with a reduction of 28.4% (from 8.8 to 6.3%). However, there was no significant decrease in the rates of IPV victimization among men between 2006 and 2012. Bidirectional violence also decreased in the 6-year period. This study also found that harmful use of alcohol was highly associated with both victimization and perpetration of IPV.
Our study showed that, even though significant reductions in violence rates were detected, most indicators remained remarkably high in 2012. Regarding IPV victimization, the comparison between the 2006 and 2012 waves found that 6% of the participants referred having suffered at least one violent event in 2012, compared to nearly 8% in 2006. The reduction of over 28% in victimization among women was perhaps the most important result of this study (8.8% in 2006 vs. 6.3% in 2012). It was also the most relevant change in this 6-year period. This is supported by a similar reduction (over 30%) in the perpetration rates among men. On the other hand, IPV rates of women against men were not significantly reduced. Combined, these findings support the hypothesis that the Maria da Penha Law might have played a role in such change. It should be noted that all campaigns and advocacy initiatives carried out in the country have focused on “violence against women,” disregarding the violence perpetrated by women against their partners. Previous studies have also reported an impact of this law, highlighting its positive aspects and pointing out its limitations, such as the lack of protective measures, material resources, and manpower, and also criticizing the fragmentation of the health care network in Brazil.13
Although our findings show a decrease in many IPV indicators, in agreement with previous studies, the youngest and less educated layers of the population still have the highest rates of IPV.9,20 This suggests that the few initiatives of IPV prevention had less of an impact on this sector of society. With respect to the distribution across Brazilian regions, our findings revealed a significant decline of perpetrators in the South (13.8 to 3.5%). Rio Grande do Sul (the most populous state in the South region) has recently developed and launched a monitoring center to tackle violence against women, implementing new advocacy, prevention, and support strategies.21 This initiative might have contributed to the steep regional reductions in IPV. Even though the results of this program were released in the same year of our data collection (2012), a few important actions of this program were actually put into place in May 2011, and our survey might have detected its impact, since the assessment focused on events occurring in the previous 12 months, which would be during year 2011.
It must be pointed that the comparison of prevalence rates between different countries or even with other Brazilian surveys is a great challenge. Methodology discrepancies, such as assessment of different types and severity of violence, different interviewing methods (phone, individual, or couples), and distinct time frames complicate comparisons.22 Accordingly, we found great discrepancies in IPV rates when comparing our results to those of recent surveys performed in the country. Previous reports have shown IPV victimization rates ranging from 18 to 44% in Brazil, with perpetration rates estimated at up to 16% in the male population9,10,23 – rates that are much higher than the ones reported here. Such differences might have resulted from the severity of the events recorded. In contrast, these estimates agree with our results when it comes to the small gap between men and women regarding IPV perpetration rates. Our results showed that perpetration rates are higher among women compared to men, and also that women seem to present higher rates of bidirectional violence compared to men (3.3 vs. 2.6% for men). Recent studies have suggested that women are equally or more likely to be the perpetrators of IPV, and that men are equally likely to be the victims of IPV.24 According to Fanslow et al.,25 a substantial proportion of women report to fight back when attacked, which could help explain the high rates of perpetration among women. Further, recent studies of IPV have been focusing on the perpetrator (men and women) and on bidirectional violence, in an attempt to understand IPV in its whole complexity.26,27
IPV was associated with harmful use of alcohol (measured by binge drinking and AUD), particularly in men (victim or perpetrator), in agreement with previous studies showing evidence that alcohol use by one or both partners contributes to the risk and severity of IPV.28,29 This result also replicates our previous publication based on the 2006 dataset alone.30 Additionally, male-to-female IPV perpetration has been consistently linked to heavy drinking by men31 and AUD.32,33 It is relevant to highlight that gender differences were not spotted with regards to perpetration of violence in our results. We also found that major predictors of IPV perpetration, such as illegal substance use (apart from sedative use), were identical between genders. Like in previous studies24,34 our findings suggest that the profile of IPV goes beyond gender differences, being more related to exposure to substance use,35,36 especially cocaine.37
The coexistence of victimization and aggression is an important issue that has received attention over the last decades. Our study showed that 2.4% of the Brazilian population reported being both victim and perpetrator of IPV in 2012, with a reduction in relation to 2006 (3.2 in 2006 vs. 2.4% in 2012). Overall, it is possible to state that all risk factors investigated in this study were strongly associated with bidirectional violence: smoking, alcohol-related problems, use of sedative and of illegal drugs. It must be highlighted that only a few studies so far have specifically investigated bidirectional violence; however, the risk factors mentioned have been identified before – such as alcohol, tobacco, and illegal drug use.29,35 Okuda et al.38 have shown that across an extensive variety of factors, the strongest association with violence perpetration is victimization itself, leading to a cycle of escalating violence. Taken together, the present results and the literature about bidirectional IPV indicate that individuals affected by bidirectional violence tend to suffer the most.
Our study has several limitations – first of all the fact that this is a study based on secondary data, since the focus of the BNADS surveys was originally to assess drug consumption, and thus specific methods to investigate interpersonal partner violence were not applied, such as interviewing couples as opposed to randomly selected individuals. In the absence of the partner, the participant may deny the incidents of IPV,39 which might have led to underreporting. Nevertheless, individual interviews have the advantage of preserving confidentiality. In turn, the format of the questionnaire, which covers events related to victimization and perpetration, tends to minimize underreporting. Further, another possible limitation is the use of CTS2, which does not cover the magnitude of all possible forms of violence committed between intimate partners, emphasizing more severe events mostly. However, the only other tool validated in Brazilian Portuguese was WHO’s Violence Against Women Instrument (VAWI), which was developed to assess violence against women only. Further, use of the CTS2 is consolidated in Brazil.40 Unfortunately the assessment of IPV by face-to-face interviewing is not ideal. However, the methodology could not be changed to self-report using sealed envelopes (as was used to guarantee confidentiality in reporting illegal drug use), because this change would prevent comparisons between the two waves of the survey. Finally, even though we benefit from the analysis of nationally representative data, it is important to bear in mind that both surveys had a cross-sectional design, which prevents conclusions regarding causality.
In conclusion, the present results provided insights regarding the magnitude, trends, and factors related to IPV in Brazil. This knowledge will be useful for the development of tailored interventions as well as evidence-based advocacy. The reduction in IPV rates, mostly in terms of female victimization, suggests a positive impact of the newly implemented Maria da Penha Law, reinforcing the idea that targeted initiatives can have an impact on this issue. However, because of its gender-specific approach, specifically targeting cases of men-perpetrator vs. women-victim, this initiative might have missed the opportunity to impact the equally high rates of violence perpetrated by women. Finally, our findings support the idea that efficient management of drug use issues in society may play a role in preventing domestic violence, especially IPV.
Acknowledgements
This study was supported by grants from Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) during the design and conduct of the survey.
References
1. Stockl H, Devries K, Rotstein A, Abrahams N, Campbell J, Watts C, et al. The global prevalence of intimate partner homicide: a systematic review. Lancet. 2013;382:859-65. [ ]
2. World Health Organization (WHO), Department of Reproductive Health and Research, London School of Hygiene and Tropical Medicine, South African Medical Research Council. Global and regional estimates of violence against women: prevalence and health effects of intimate partner violence and non-partner sexual violence. Geneva: WHO; 2013. [ ]
3. Weinsheimer RL, Schermer CR, Malcoe LH, Balduf LM, Bloomfield LA. Severe intimate partner violence and alcohol use among female trauma patients. J Trauma. 2005;58:22-9. [ ]
4. Cho H, Velez-Ortiz D, Parra-Cardona JR. Prevalence of intimate partner violence and associated risk factors among Latinos/as: an exploratory study with three Latino subpopulations. Violence Against Women. 2014;20:1041-58. [ ]
5. Pontecorvo C, Mejia R, Aleman M, Vidal A, Majdalani MP, Fayanas R, et al. [Detection of domestic violence against women. Survey in a primary health care clinic]. Medicina (B Aires). 2004;64:492-6. [ ]
6. Carrasco-Portino M, Vives-Cases C, Gil-Gonzalez D, Alvarez-Dardet C. [What do we know about men who abuse their female partner? A systematic review]. Rev Panam Salud Publica. 2007;22:55-63. [ ]
7. Garcia LP, de Freitas LR, da Silva GD, Höfelmann DA. [Corrected estimates of femicides in Brazil, 2009 to 2011]. Rev Panam Salud Publica. 2015;37:251-7. [ ]
8. Waiselfisz JJ, Ribeiro C. Mapa da violência 2012. Caderno complementar 1: Homicídio de mulhers no Brasil [Internet]. São Paulo: Instituto Sangari. 2011 [cited 2016 Mar 11]. mapadaviolencia.org.br/pdf2012/mapa2012_mulher.pdf [ ]
9. Brasil, Senado Federal. Violência doméstica e familiar contra a mulher [Internet]. Mar 2013 [cited 2016 Mar 11]. http://www.senado.gov.br/senado/datasenado/pdf/datasenado/DataSenado-Pesquisa-Violencia_Domestica_contra_a_Mulher_2013.pdf [ ]
10. Instituto Avon. Instituto Avon/Data Popular: Percepções dos homens sobre a violência doméstica contra a mulher [Internet]. [cited 2016 Mar 11]. compromissoeatitude.org.br/wp-content/uploads/2013/12/folderpesquisa_instituto22x44_5.pdf [ ]
11. Schraiber LB, D’Oliveira AF, França Junior I; Grupo de Estudos em População, Sexualidade e Aids. [Intimate partner sexual violence among men and women in urban Brazil, 2005]. Rev Saude Publica. 2008;42:127-37. [ ]
12. Zaleski M, Pinsky I, Laranjeira R, Ramisetty-Mikler S, Caetano R. Intimate partner violence and alcohol consumption. Rev Saude Publica. 2010;44:53-9. [ ]
13. Meneghel SN, Mueller B, Collaziol ME, de Quadros MM. [Repercussions of the Maria da Penha law in tackling gender violence]. Cien Saude Colet. 2013;18:691-700. [ ]
14. Overup CS, DiBello AM, Brunson JA, Acitelli LK, Neighbors C. Drowning the pain: intimate partner violence and drinking to cope prospectively predict problem drinking. Addictt Behav. 2015;41:152-61. [ ]
15. Weiss NH, Duke AA, Sullivan TP. Probable posttraumatic stress disorder and women’s use of aggression in intimate relationships: the moderating role of alcohol dependence. J Trauma Stress. 2014;27:550-7. [ ]
16. Rada C. Violence against women by male partners and against children within the family: prevalence, associated factors, and intergenerational transmission in Romania, a cross-sectional study. BMC Public Health. 2014;14:129. [ ]
17. Zaha R, Helm S, Baker C, Hayes D. Intimate partner violence and substance use among Hawai’i youth: an analysis of recent data from the Hawai’i Youth Risk Behavior Survey. Subst Use Misuse. 2013;48:11-20. [ ]
18. Straus MA, Hamby SL, Boney-McCoy S, Sugarman DB. The Revised Conflict Tactics Scales (CTS2). J Fam Issues. 1996;17:283-316. [ ]
19. Quintana MI, Andreoli SB, Jorge MR, Gastal FL, Miranda CT. The reliability of the Brazilian version of the Composite International Diagnostic Interview (CIDI 2.1). Braz J Med Biol Res. 2004;37:1739-45. [ ]
20. Stockman JK, Lucea MB, Bolyard R, Bertand D, Callwood GB, Sharps PW, et al. Intimate partner violence among African American and African Caribbean women: prevalence, risk factors, and the influence of cultural attitudes. Global Health Action. 2014;7:24772. [ ]
21. Comissão de Cidadania e Direitos Humanos, Assembleia Legislativa do Rio Grande do Sul. Relatório Lilás [Internet]. 2013 Nov 27 [cited 2016 Mar 11]. direitos-humanos-alrs.blogspot.com.br/2013/11/relatorio-lilas.html [ ]
22. McLaughlin J, O’Carroll RE, O’Connor RC. Intimate partner abuse and suicidality: a systematic review. Clin Psychol Rev. 2012;32:677-89. [ ]
23. Serviço social do Comércio (SESC), Fundação Perseu Abramo. Mulheres brasileiras e gênero nos espaços público e privado [Internet]. 2010 Aug [cited 2016 Mar 11]. novo.fpabramo.org.br/sites/default/files/pesquisaintegra.pdf [ ]
24. Ulloa EC, Hammett JF. The effect of gender and perpetrator-victim role on mental health outcomes and risk behaviors associated with intimate partner violence. J Interpers Violence. 2016;31:1184-207. [ ]
25. Fanslow JL, Gulliver P, Dixon R, Ayallo I. Hitting back: women’s use of physical violence against violent male partners, in the context of a violent episode. J Interpers Violence. 2015;30:2963-79. [ ]
26. Testa M, Hoffman JH, Leonard KE. Female intimate partner violence perpetration: stability and predictors of mutual and nonmutual aggression across the first year of college. Aggress Behav. 2011;37:362-73. [ ]
27. Heslop J, Banda R. Moving beyond the “male perpetrator, female victim” discourse in addressing sex and relationships for HIV prevention: peer research in Eastern Zambia. Reprod Health Matters. 2013;21:225-33. [ ]
28. Caetano R, Cunradi CB, Clark CL, Schafer J. Intimate partner violence and drinking patterns among white, black, and Hispanic couples in the U.S. J Subst Abuse. 2000;11:123-38. [ ]
29. Cunradi CB. Drinking level, neighborhood social disorder, and mutual intimate partner violence. Alcohol Clin Exp Res. 2007;31:1012-9. [ ]
30. Zaleski M, Pinsky I, Laranjeira R, Ramisetty-Mikler S, Caetano R. Intimate partner violence and contribution of drinking and sociodemographics: the Brazilian National Alcohol Survey. J Interpers Violence. 2010;25:648-65. [ ]
31. Bazargan-Hejazi S, Kim E, Lin J, Ahmadi A, Khamesi MT, Teruya S. Risk factors associated with different types of intimate partner violence (IPV): an emergency department study. J Emerg Med. 2014;47:710-20. [ ]
32. Testa M, Kubiak A, Quigley BM, Houston RJ, Derrick JL, Levitt A, et al. Husband and wife alcohol use as independent or interactive predictors of intimate partner violence. J Stud Alcohol Drugs. 2012;73:268-76. [ ]
33. Wilsnack SC, Wilsnack RW, Kantor LW. Focus on: women and the costs of alcohol use. Alcohol Res. 2013;35:219-28. [ ]
34. Watkins LE, Maldonado RC, DiLillo D. Hazardous alcohol use and intimate partner aggression among dating couples: the role of impulse control difficulties. Aggress Behav. 2014;40:369-81. [ ]
35. Afifi TO, Henriksen CA, Asmundson GJ, Sareen J. Victimization and perpetration of intimate partner violence and substance use disorders in a nationally representative sample. J Nerv Ment Dis. 2012;200:684-91. [ ]
36. Kraanen FL, Vedel E, Scholing A, Emmelkamp PM. Prediction of intimate partner violence by type of substance use disorder. J Subst Abuse Treat. 2014;46:532-9. [ ]
37. Mattson RE, O’Farrell TJ, Lofgreen AM, Cunningham K, Murphy CM. The role of illicit substance use in a conceptual model of intimate partner violence in men undergoing treatment for alcoholism. Psychol Addict Behav. 2012;26:255-64. [ ]
38. Okuda M, Olfson M, Wang S, Rubio JM, Xu Y, Blanco C. Correlates of intimate partner violence perpetration: results from a National Epidemiologic Survey. J Trauma Stress. 2015;28:49-56. [ ]
39. Caetano R, Field C, Ramisetty-Mikler S, Lipsky S. Agreement on reporting of physical, psychological, and sexual violence among white, black, and Hispanic couples in the United States. J Interpers Violence. 2009;24:1318-37. [ ]
40. Viana MC, Teixeira MG, Beraldi F, Bassani Ide S, Andrade LH. Sao Paulo Megacity Mental Health Survey – a population-based epidemiological study of psychiatric morbidity in the Sao Paulo metropolitan area: aims, design and field implementation. Rev Bras Psiquiatr. 2009;31:375-86. [ ]
Received: August 16, 2015; Accepted: February 3, 2016
 This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.